 Oct. 28, 2012
Oct. 28, 2012
Gastric cancer (GC) is the fourth most common cancer in the world and the second leading cause of cancer-related death. In Australia, the age standardised incident rate (ASR) is 9-10 per 100,000 people and over 11,000 deaths were recorded between 1996 and 2006. The current diagnostic strategy for GC is inadequate.
The ability to detect early stage GC increases the expected five-year survival rate (5-YSR) after symptoms of GC appear from 10-30%, to a 5-YSR for those diagnosed at early stage GC >50%. A reliable, cost-effective screening test for the early detection of GC therefore has considerable clinical potential. Particularly in geographic regions including China, Hong Kong, Japan, Korea, Central Europe, Scandinavia, South and Central America and Russia which have a far higher incidence of and mortality from GC.
Researchers at the University of Adelaide have identified 4 candidate markers for gastric cancer that can be measured from patient blood serum. As can be seen in the table below, the pattern of expression of these 4 markers can be used to identify the presence and nature of gastrointestinal disease. Further, these markers have been shown to have the potential to more accurately segregate GC patients from health controls, and patients with benign gastrointestinal diseases. From the ROC curves, the AUC values indicate that the markers can be used to distinguish the following:
Marker | Distinguishes Between | Accuracy (AUC) | Purpose |
Haptoglobin | GC from Healthy Healthy from Benign | 0.86 1.00 | Detecting GC |
Vitamin D Binding Protein | GC from Healthy GC from Benign | 1.00 0.84 | Removing Benign False Positives |
Afamin | GC from Healthy Healthy from Benign | 0.98 0.94 | Removing Healthy |
Clusterin | GC from Healthy GC from Benign | 0.93 0.94 | Determining GC from Healthy and Benign |
These four markers can be combined for a rapid and cost-effectivescreening testfor GC. Patients identified as at risk using this test can be referred for endoscopic biopsy and histopathology.
This technology is for four (4) serum biomarkers that are potentially useful as part of a diagnostic screening test for early stage GC.
Cohort demographics
Serum samples were obtained from preoperative GC patients with intestinal type gastric adenocarcinoma (according to Lauren classification). This included early-stage gastric cancer (AJCC 6th Edition Stage I disease, with minimal depth of invasion into mucosa and no metastatic lymph nodes). These were compared with non-metastatic benign gastrointestinal disease serum samples which were non-metastatic. These in turn were compared with healthy control samples. All clinical data was collected by gastroenterologists and stages conformed by histopathology. Clinical information regarding gastritis status andH. pyloriinfection and atrophy were also obtained in all samples.
Figure 1A
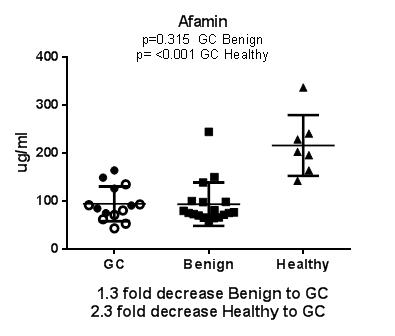
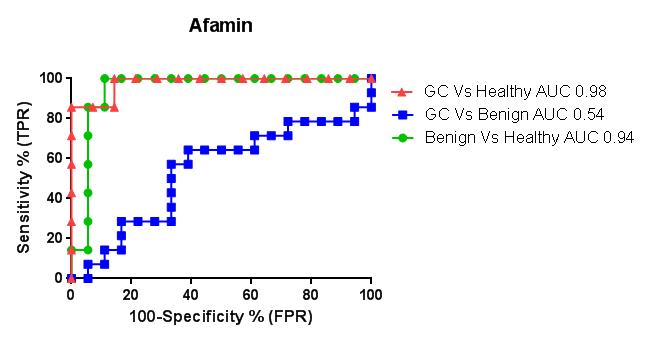
Figure 1B
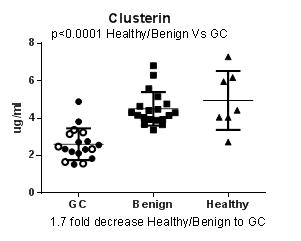
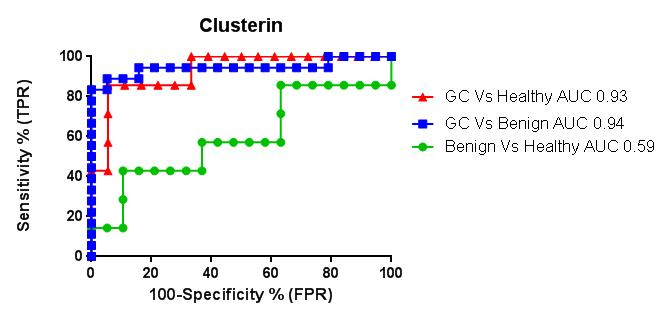
Figure 1C
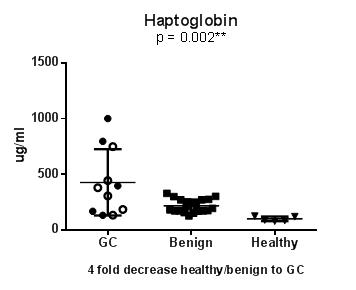
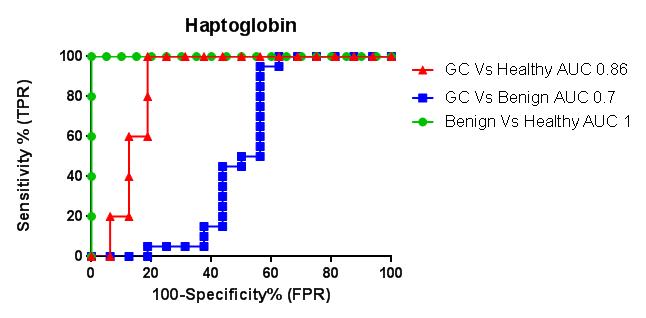
Figure 1D
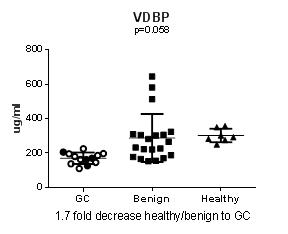
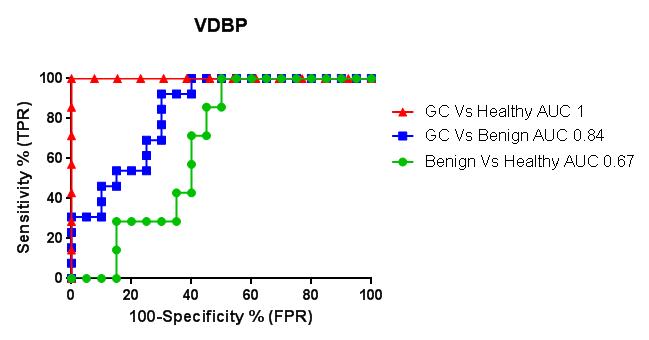
Figure 1A to 1D: Graphical representation and ROC curves of analyses comparing serum from patient with gastric cancer including early stage (open circles), benign gastrointestinal disease, and healthy serum, comparing the three combinations, indicating accuracy (AUC), true positive rate (sensitivity) and false positive rate (100%-specificity).
Elisa Results
Compared to sera that was as closely as possible matched fro age and gender from patients with benign gastrointestinal disease without intestinal metaplasia, and from healthy controls we found serum from patients with GC to have
- down regulation of afamin 1.3 fold, p=0.315 from benign to GC, and 2.3 fold, p<0.001** from healthy to GCFigure 1A
- down regulation of clusterin 1.7 fold, p<0.001**Figure 1B
- up-regulation of haptoglobin 1.7 fold, p=0.024*Figure 1C
- down regulation of VDBP 1.7 fold, p=0.058Figure 1D
Furthermore, the levels of these four serum proteins in the 11 early stage GC samples were indistinguishable from those in the advanced stage GC samples (Figures 1A-D, open circles). Collectively, these findings suggest that these 4 proteins could service as promising biomarkers for the detection of early-stage GC.
Comparison with existing diagnostics
Existing clinical biomarkers (CA 19-9, CEA and CA 72-4) are neither sufficiently sensitive nor specific for routine screening and are primarily used to monitor disease progression. The sensitivity of CEA, CA19-9 and CA72-4 has been estimated to be as low as 33% in patients with GC across a number of studies, making them unsuitable for early detection. In comparison, the 4 biomarkers we have identified for early GC and that we wish to take into Phase II of a Biomarker Trial have been shown in literature published by our group to more accurately segregate GC patients from healthy controls (Pennoet al., 2012 J Prot 77:40-58).
Current Research
We have established a strong collaboration with the National University Hospital in Singapore and now have access to serum from both early and late stage gastric cancer patients as well as from benign gastrointestinal disease patients, which can be used as controls. We are currently performing further assay validation of this large sample cohort and expect to have further results regarding the biomarkers' sensitivity and specificity in the South East Asian sample during 2015.
Outcome of clinical use of this screening tool
Thepotentialapplications of this technologyare in the development of a viable rapidand cost-effective diagnostic testfor early stage gastric cancer.Patients identified as at risk using this test can be referred for further assessment through endoscopic biopsy and histopathology. This will allow for earlier detection and treatment of gastric cancer and reduce the number of patients who are unnecessarily sent for invasive and expensive endoscopic assessment.
The potential applications of this technology are in the development of a viable rapid and cost-effective diagnostic test for early stage gastric cancer. This technology will therefore be of interest to companies in the diagnostics field, already have a presence in the gastric or oncology space or who manufacture ELISA kits and wish to enter the diagnostics market.
由于技术保密工作限制,技术信息无法完全展现,请通过邮箱或短信联系我们,获取更多技术资料。
metastatic lymph nodes
gastritis status andh
true positive rate
false positive rate
matched fro age

![]()
![]()
![]()

 Premium
Premium